For healthcare professionals only.

For healthcare professionals only.

BMI = the weight in kilograms divided by the square of the height in metres (kg/m2).
Caucasian, Europid, and North American ethnicity
| Classification | BMI (kg/m2) |
|---|---|
Underweight | < 18.5 |
Normal range | ≥ 18.5 and < 25.0 |
Overweight | ≥ 25.0 and < 30.0 |
Obesity | ≥ 30.0 |
Obesity, class I | ≥ 30.0 and < 35.0 |
Obesity, class II | ≥ 35.0 and < 40.0 |
Obesity, class III | ≥ 40.0 and < 50.0 |
Obesity, class IV | ≥ 50.0 and < 60.0 |
Obesity, class V | ≥ 60.0 |
South-, Southeast-, or East Asian ethnicity
| Classification | BMI (kg/m2) |
|---|---|
Underweight | < 18.5 |
Normal range | ≥ 18.5 and < 23.0 |
Overweight—At risk | ≥ 23.0 and < 25.0 |
Overweight—Moderate risk |
≥ 25.0 and < 30.0 |
Overweight—Severe risk |
≥ 30.0 |
Waist circumference provides additional information regarding cardiometabolic risk.8
Waist circumference risk threshold:
Predominant Ethnicity | Increased Abdominal Adiposity / Cardiovascular Risk | Significant Abdominal Adiposity / Greater Cardiovascular Risk | ||
| Female | Male | Female | Male |
Caucasian Europid, United States, Mid-East Mediterranean | 80 |
94 | 88 | 102 |
Latino Central, South American | 83 | 88 | 90 | 94 |
Sub-Saharan African | 80 | 94 | - | - |
African American | 90 | 80 | 99 | 95 |
African | 71.5 |
76.5 | 81.5 | 80.5 |
Asian | 80 |
85 | - | - |
Chinese | 81 |
83 | - | - |
Korean | 75 |
80 | 85 | 90 |
Canadian Aboriginal | 80 | 94 | - | - |
WOF (World Obesity Federation):
The World Obesity Federation takes the position that obesity is a chronic, relapsing, progressive disease process and emphasises the need for immediate action and the prevention and control of this global epidemic. 13
TOS (The Obesity Society):
It is the official position of The Obesity Society that obesity should be declared a disease. 10
AACE (American Association of Clinical Endocrinologists):
"[Obesity] must be viewed as a chronic disorder that essentially requires perpetual care, support, and follow-up." 11
CMA (Canadian Medical Association):
"It is important for health care providers to recognize obesity as a disease so preventive measures can be put in place..." 12
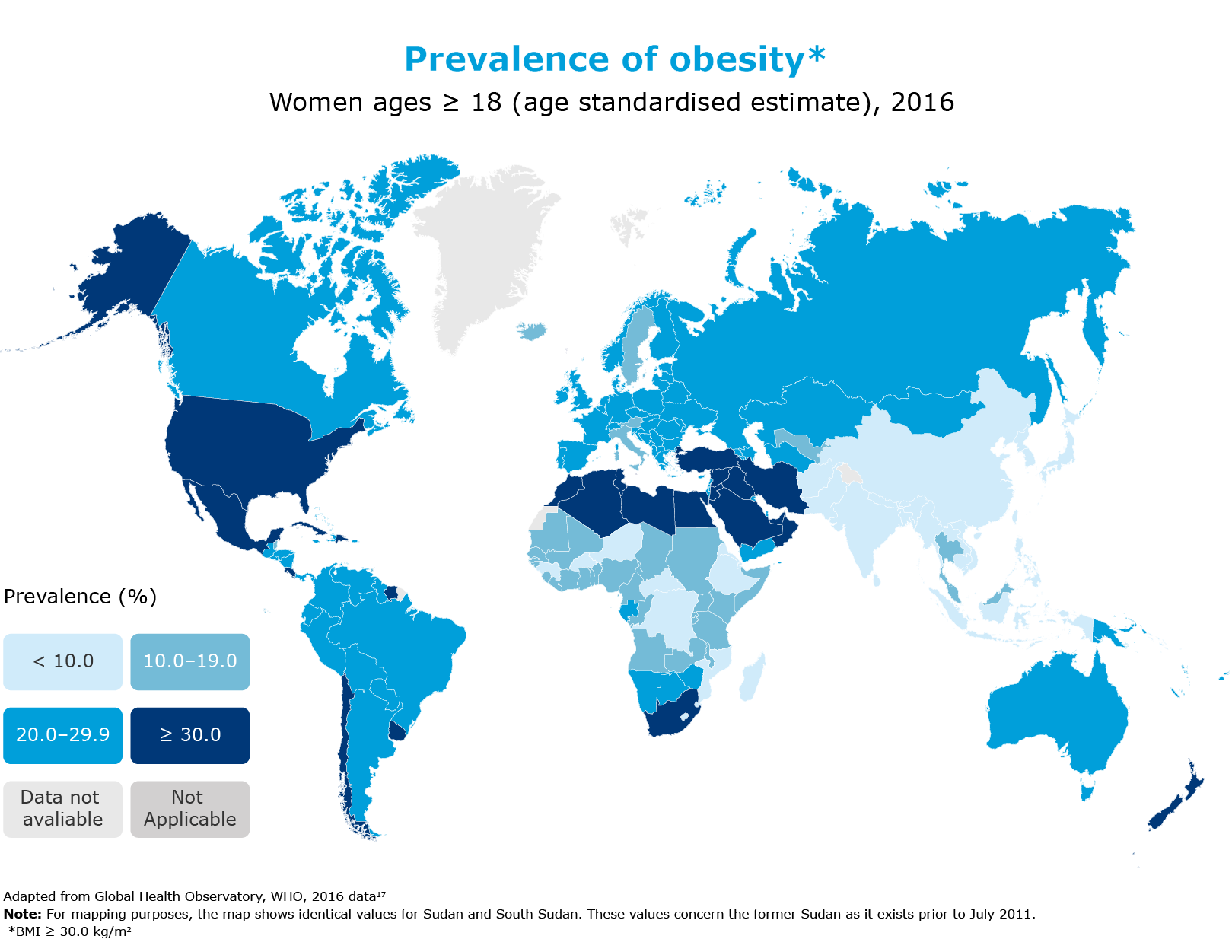
The global prevalence of obesity has nearly tripled since 1975. In 2016, more than 1.9 billion adults aged ≥ 18 were overweight. In the same year, 39% of adults aged ≥ 18 were living with overweight, and 13% were living with obesity.16
Compared to a person with overweight, class I obesity is associated with a:21

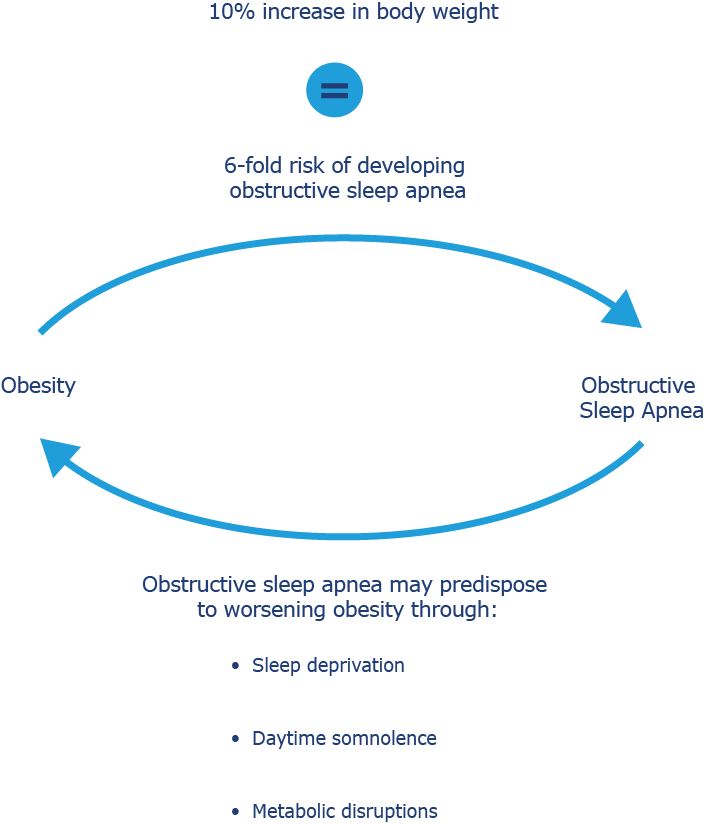
Canadians with obstructive sleep apnea are more likely to have diabetes, hypertension, heart disease and mood disorders.26
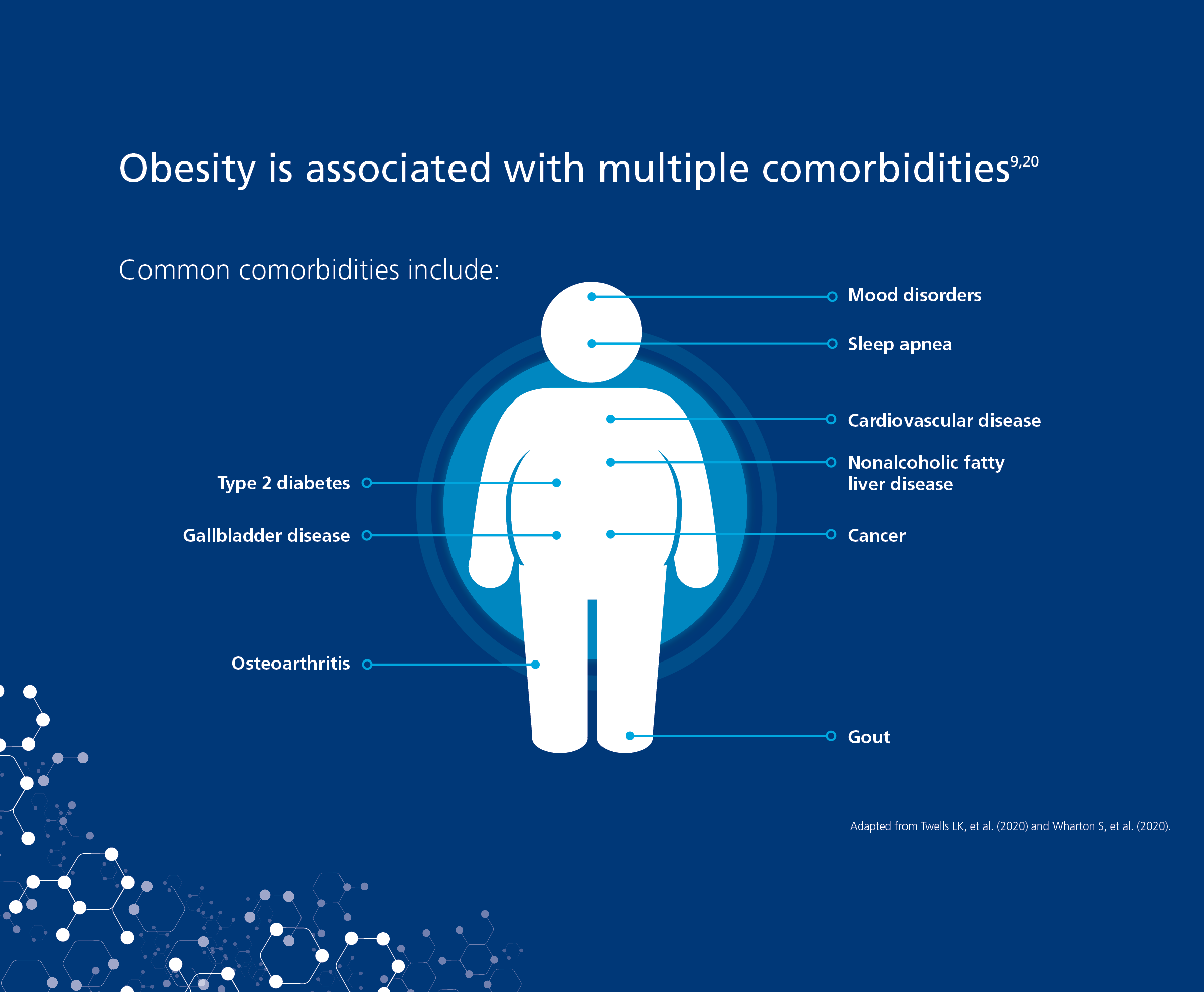
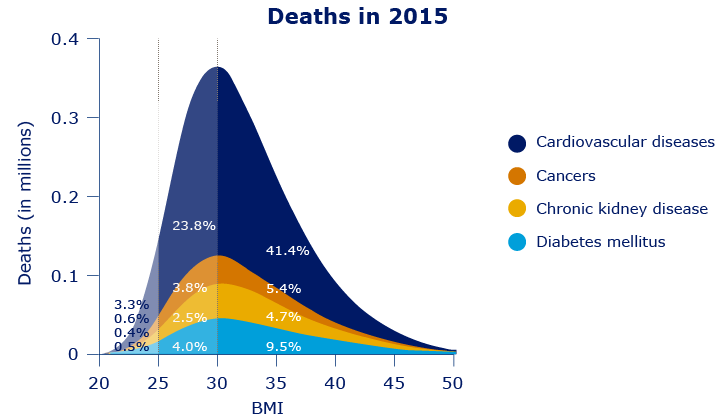
Globally, cardiovascular disease is the leading cause of mortality in people with obesity.27

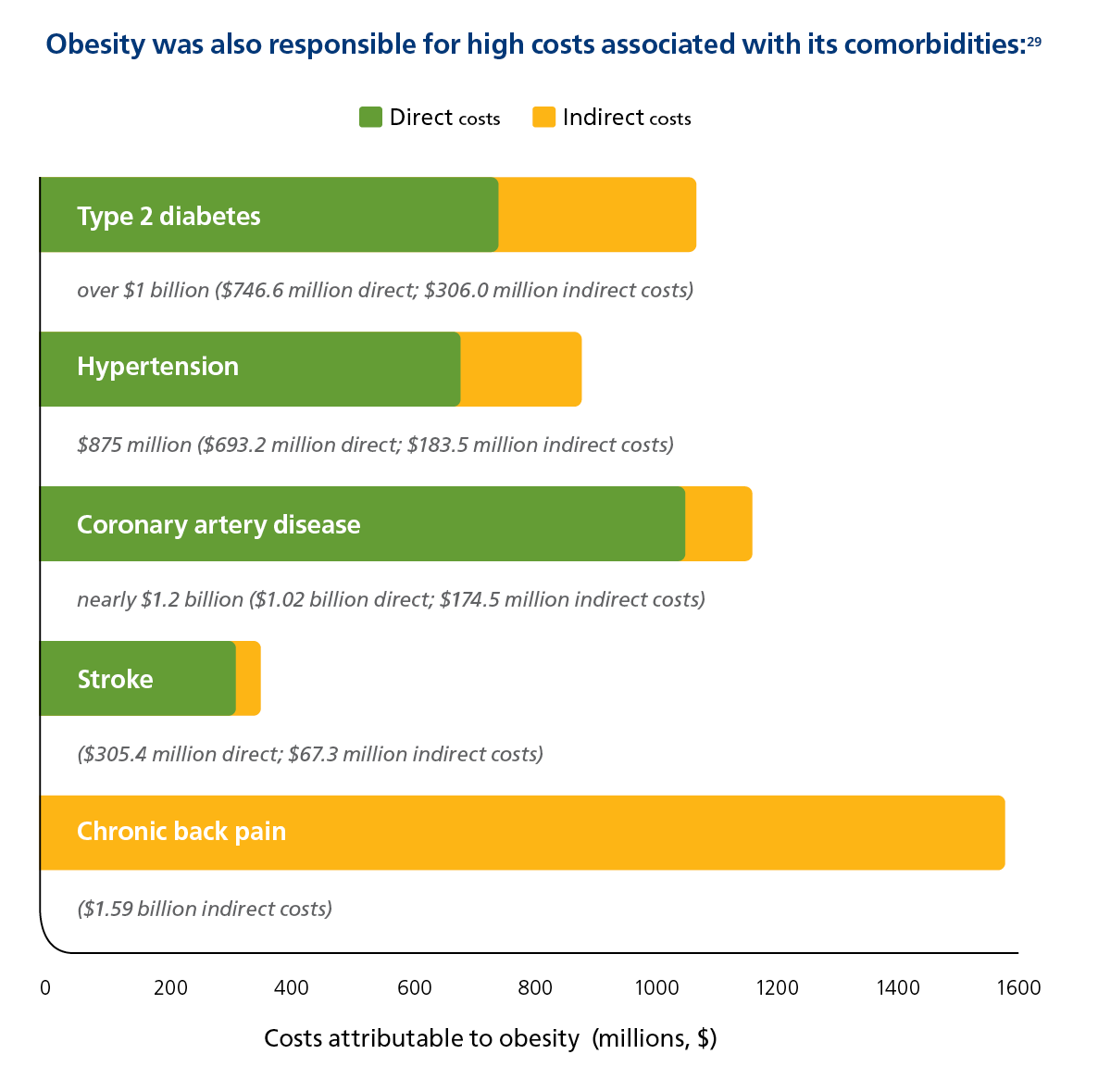
Obesity was also responsible for high costs associated with its comorbidities29
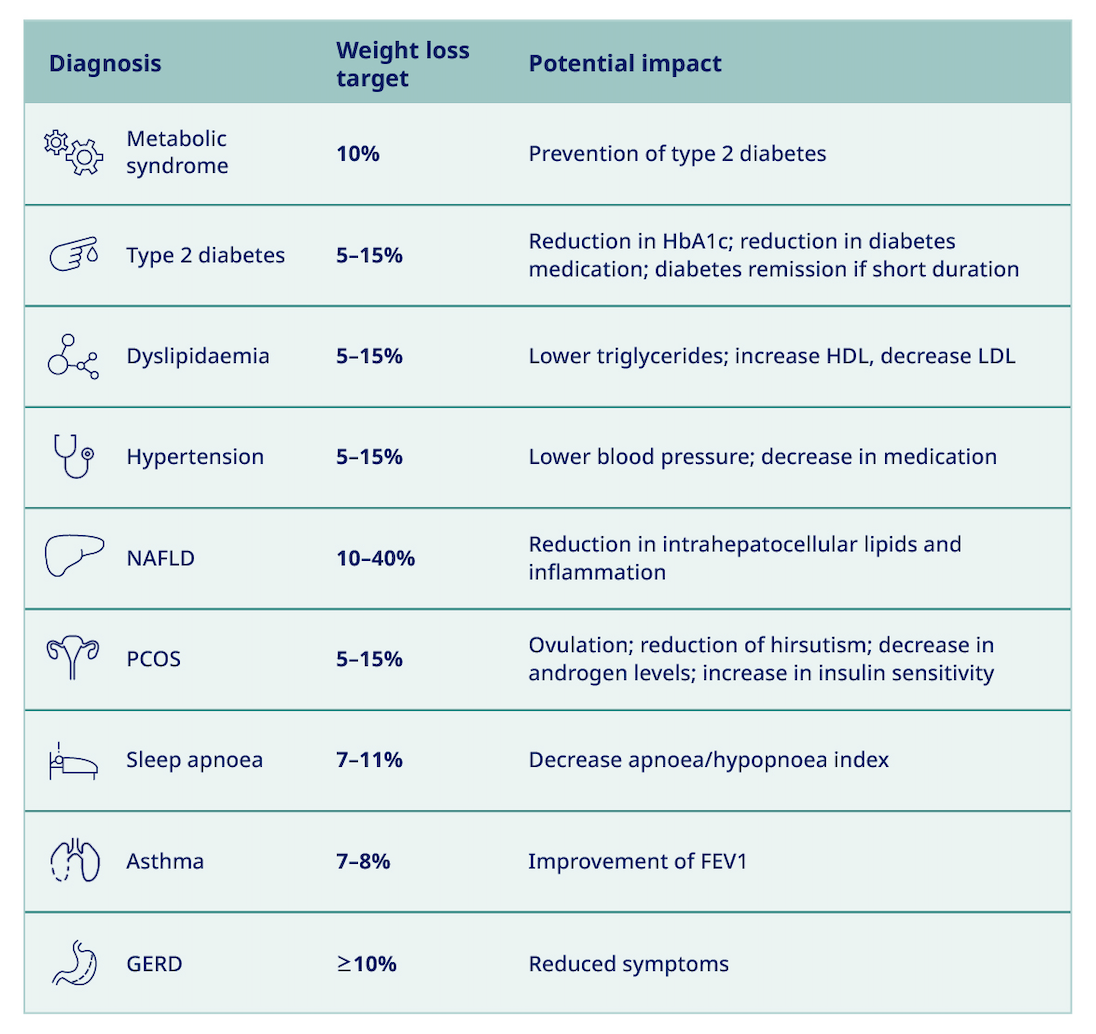
How could weight loss, achieved through behavioural treatment, impact patients with the following conditions?
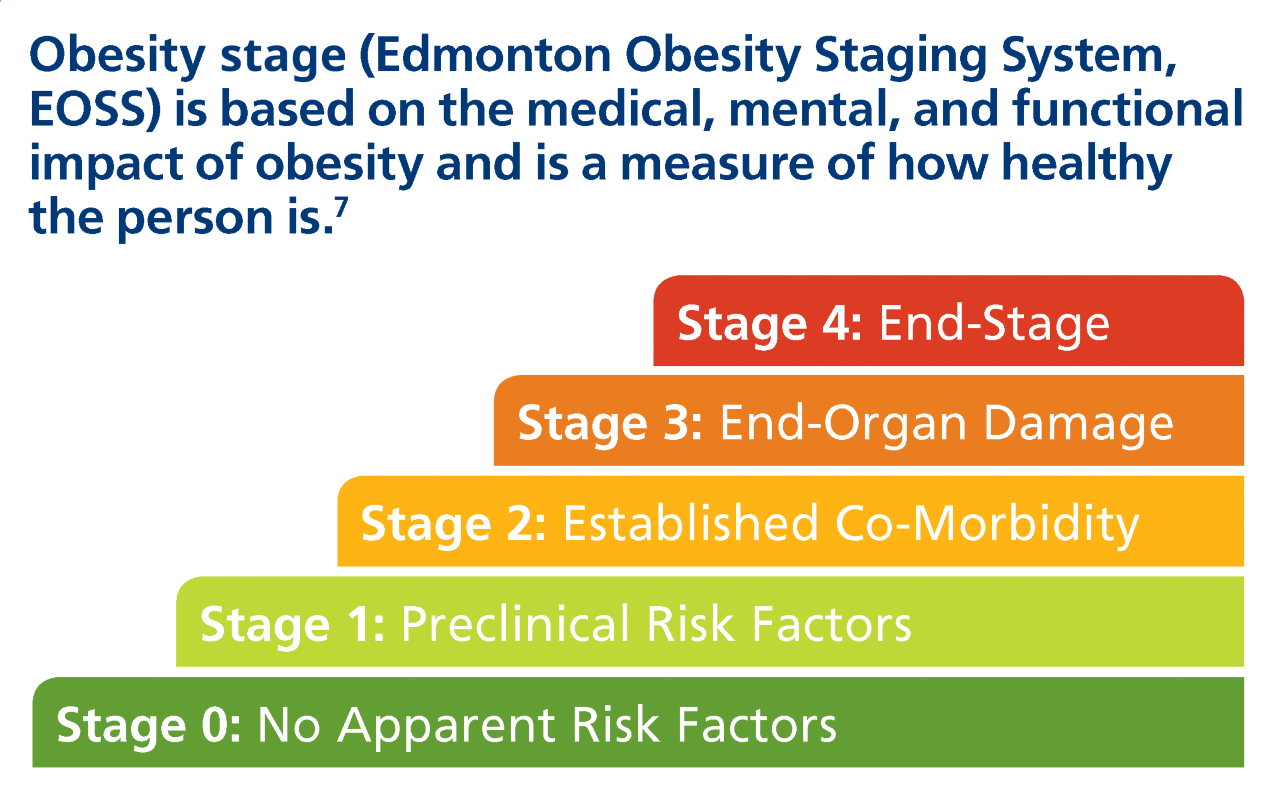
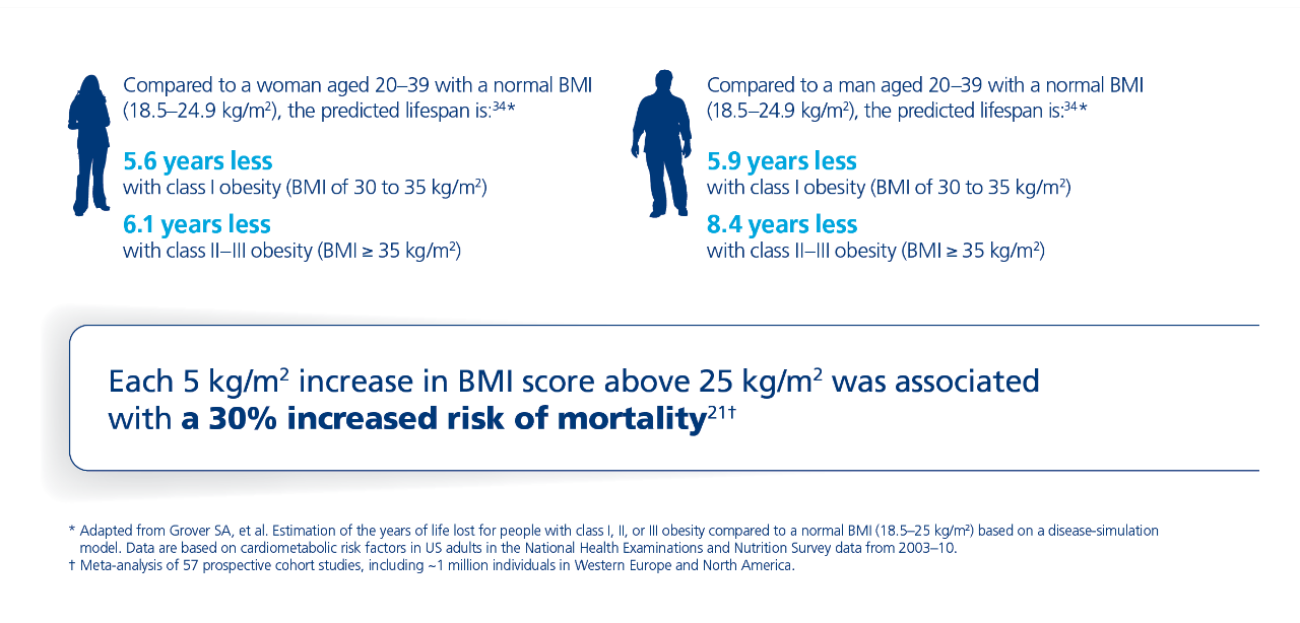
Risk of mortality is significantly increased and quality of life is significantly decreased due to obesity.
 - Udpate-1.png)
2- Update-1.png)
3 - Update-1.png)
BP, blood pressure; CV, cardiovascular; DBP, diastolic blood pressure; A1C, glycated haemoglobin; HDL, high density lipoprotein; SBP, systolic blood pressure.
A weight loss of around 7% has shown a reduction in the incidence of type 2 diabetes by 58%30†
Every 1 kg of weight loss can decrease LDL levels by 8%36
Achieving 5–10% weight loss can lead to a 30% reduction of sleep apnea symptoms26‡
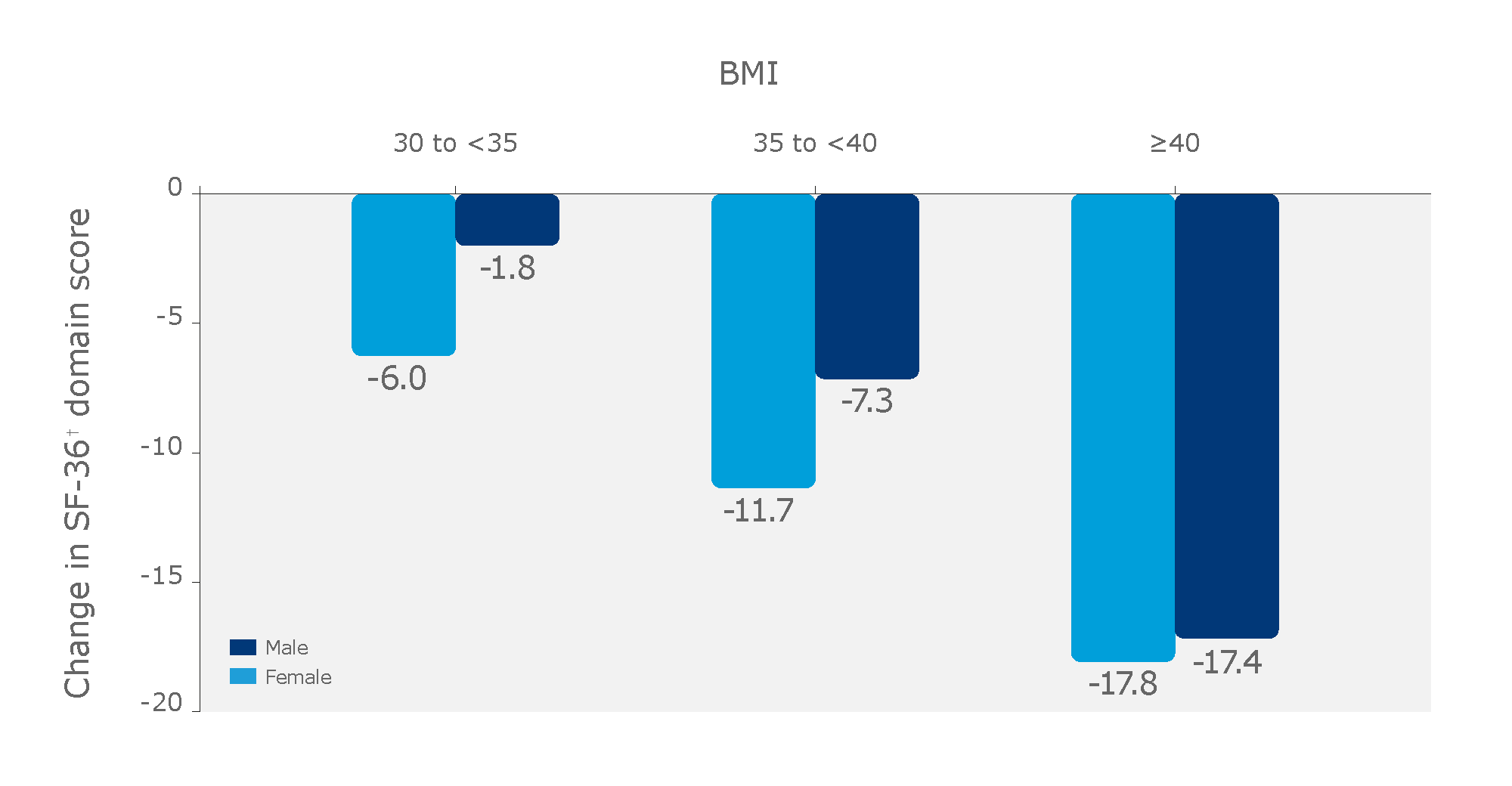
The higher the BMI, the greater the risk of impaired physical functioning, which may include limitations in mobility activities such as walking and dressing.37
Obesity has a negative impact on physical functioning compared with normal weight (BMI 18.5–24.9 kg/m2)38
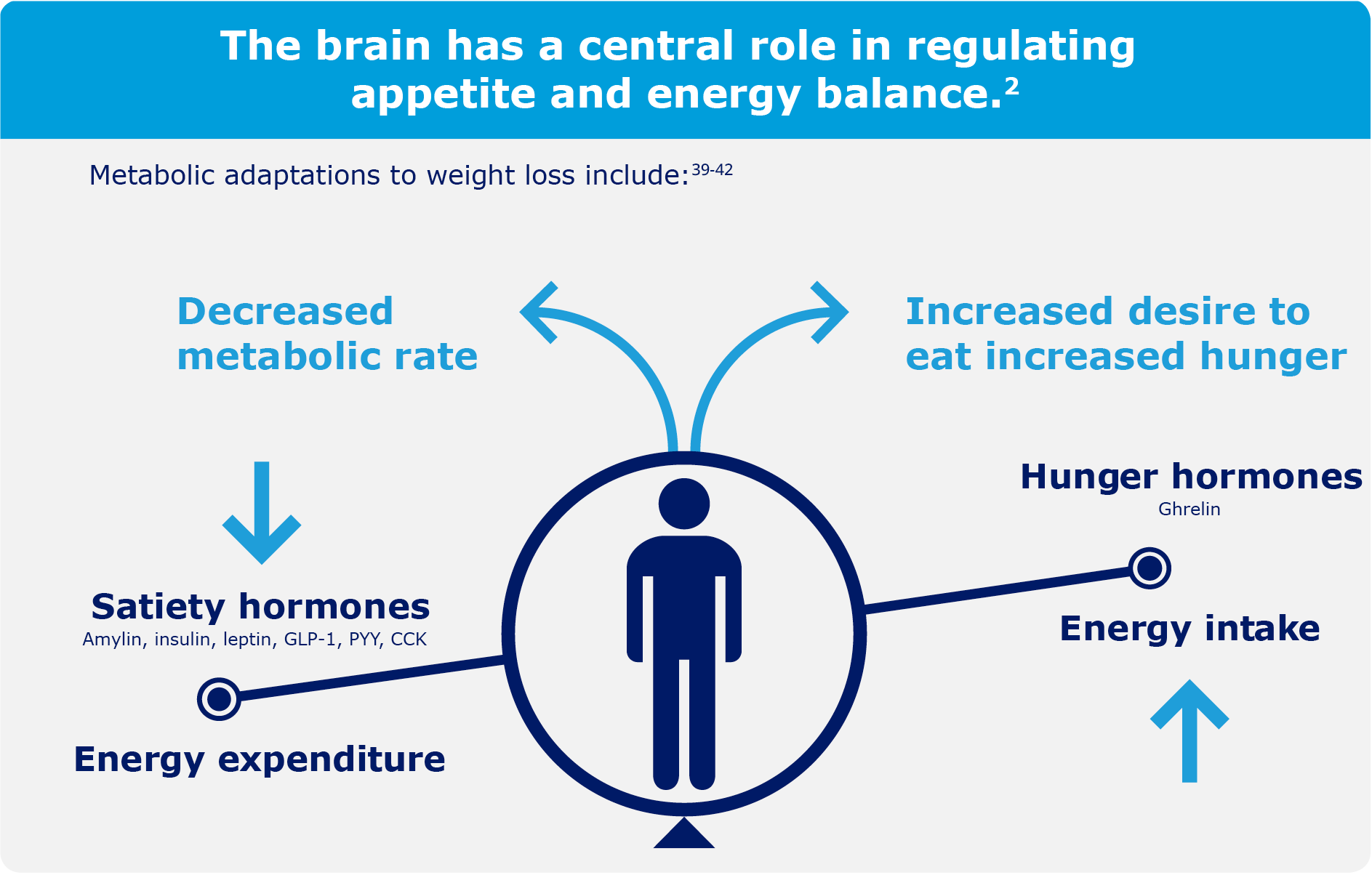
Science has discovered that physiological responses to weight loss trigger weight regain.
Weight loss in people living with obesity has been shown to cause changes in appetite hormones that increase hunger and the desire to eat for at least 1 year.39
Multiple hormones, such as ghrelin, GLP-1, and leptin, play an important role in regulating appetite.2
A review of 14 long-term studies showed that participants regained weight after weight loss achieved by dieting.43
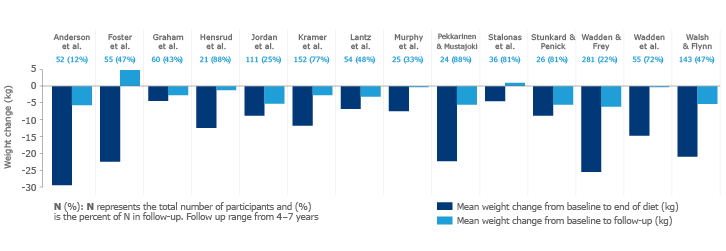
“…the high rate of relapse among people with obesity who have lost weight has a strong physiological basis and is not simply the result of the voluntary resumption of old habits."39
Behavioural interventions including medical nutrition therapy, physical activity, and cognitive-behavioural therapy are recommended as the first-line treatment option for people living with overweight or obesity to achieve clinically important weight loss and reduce obesity-related symptoms.9 Other treatment options such as pharmacotherapy and bariatric surgery may be appropriate adjunct treatments for certain people living with obesity.9
The ACTION (Awareness, Care and Treatment of Obesity MaNagement) Study is the first Canada-wide study that investigated the perceptions, attitudes, and perceived barriers to obesity management among Canadian people living with obesity (PwO), healthcare professionals (HCPs), and employers. The study was conducted through an online survey between August and October of 2017. The findings of this study highlight the misunderstanding and communication gaps that exist between these groups.44
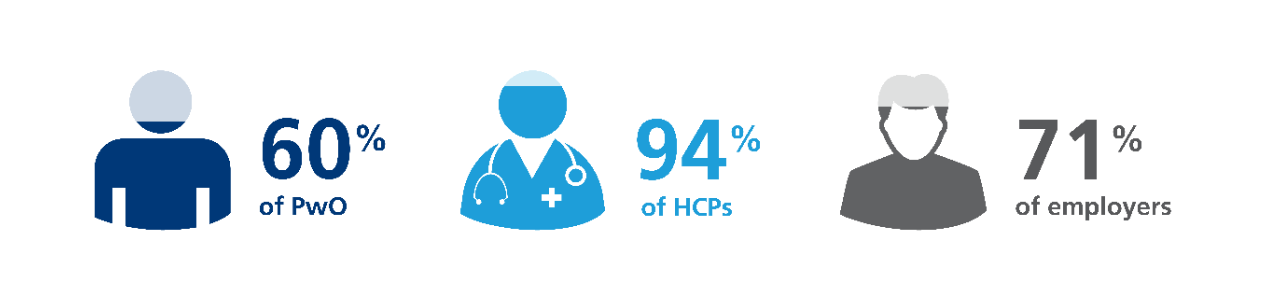
The majority of the 2545 survey respondents* agreed with the statement that “obesity is a chronic medical condition”.44
74% of PwO reported that they believe obesity has a large impact on overall health.
81% of PwO agreed that it would be beneficial to their health to lose 5–10% of their body weight.
Selected outcomes of the ACTION Study can be grouped into the following topics:44
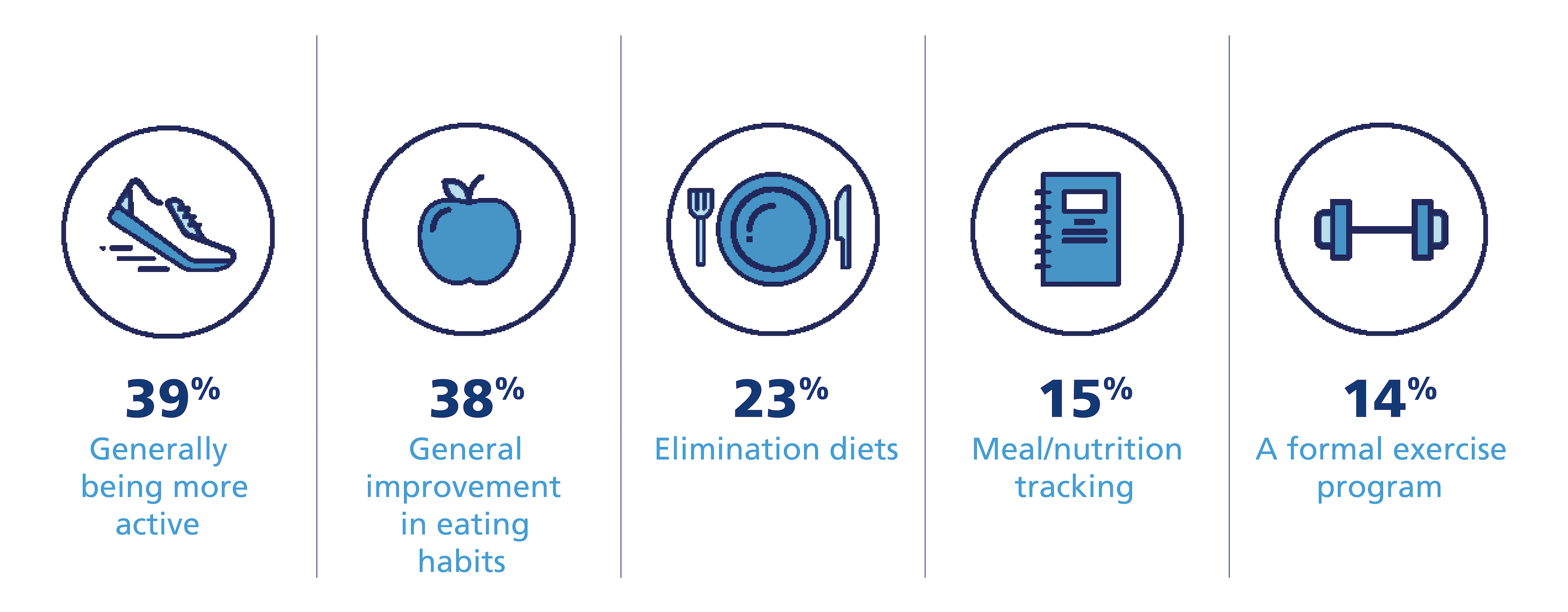
The general group of PwO reported engaging in several weight loss attempts.44
The most highly utilized methods for weight loss reported by PwO were:44*
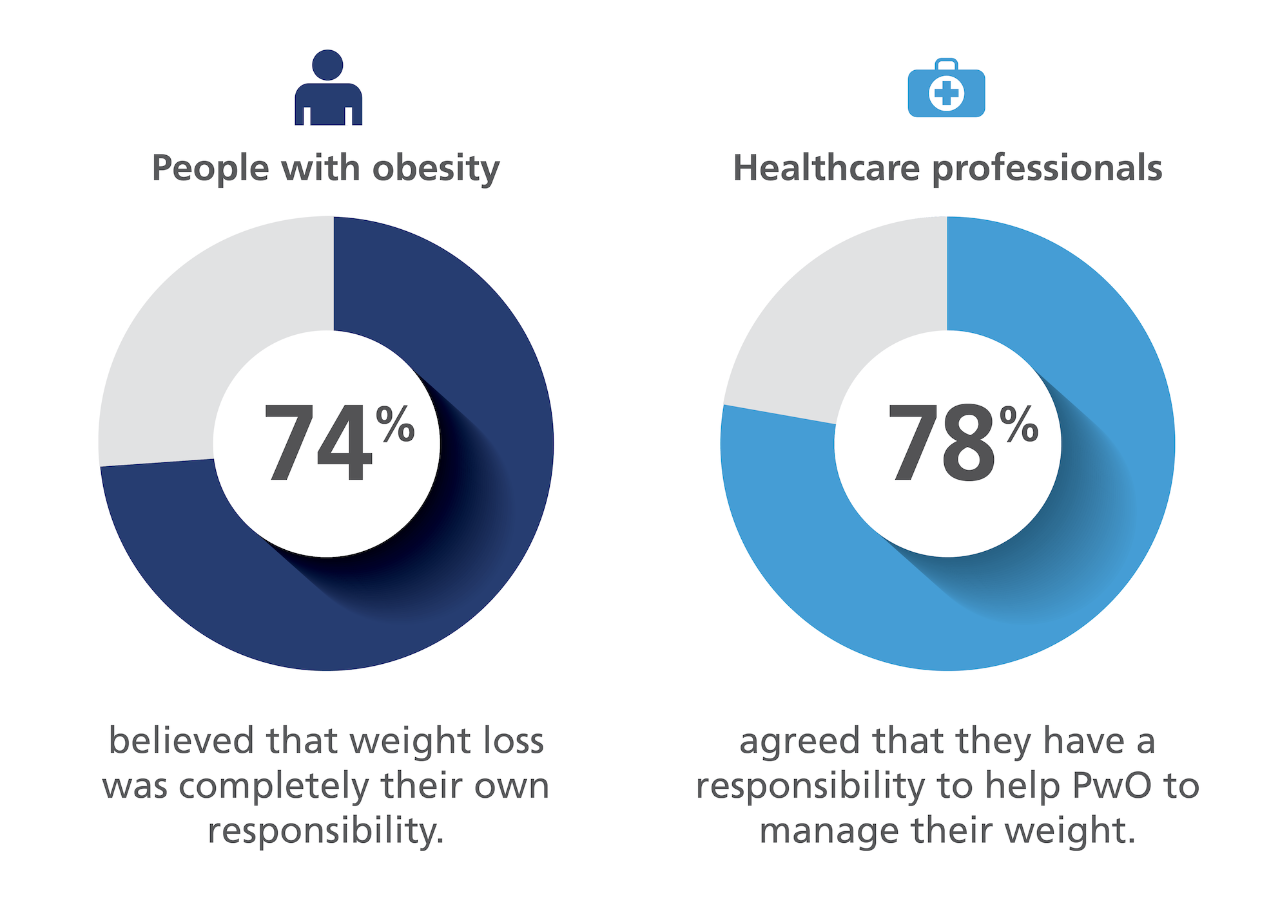
The results of the ACTION Study indicated that most people living with obesity (74%) considered weight loss to be completely their own responsibility.44
The median age at which PwO reported first struggling with excess weight was 28 years, while they reported first discussing weight with their HCP at a median age of 39 years.
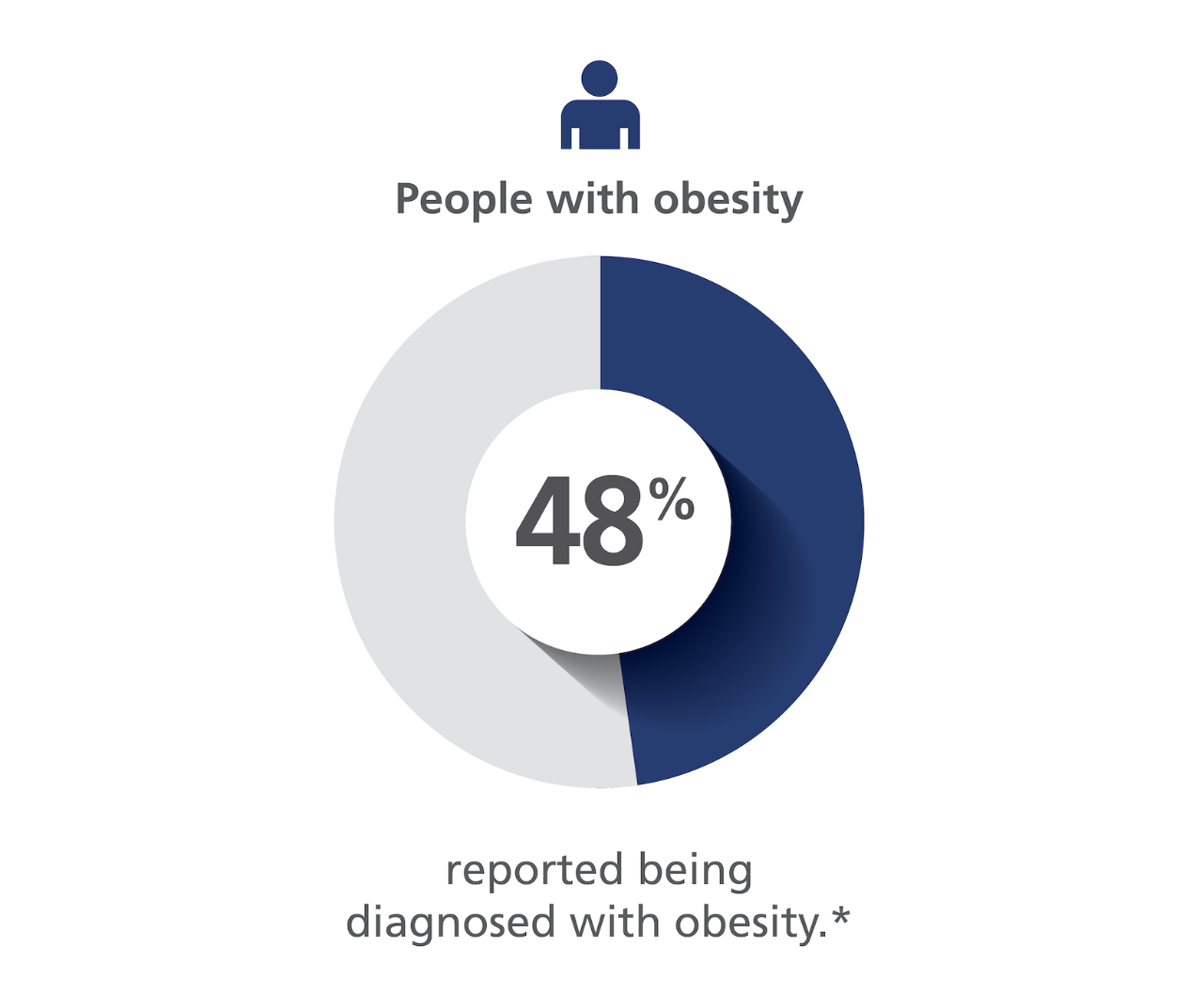
Many PwO (52%) indicated that they had not received a formal diagnosis of obesity.46
Although 72% of HCPs reported discussing weight with their patients who are in need of weight management, only 54% of PwO reported that they have had such discussions in the previous 5 years.
A gap in the patient-provider dialogue was identified, whereby HCPs reported having discussions about weight management with 72% of their patients, but only 54% of PwO reported having these discussions in the past 5 years.44

A delay of more than 10 years was reported from the time that PwO first started struggling with excess weight to the time they first discussed weight with their HCP.

Only 28% of PwO who reported having a discussion about weight with their HCP said that a weight-related follow-up appointment or call was scheduled.

PwO who reported success in losing weight engaged in discussions with their HCPs earlier than those who had no current weight loss success (median: 5 vs. 12 years).
A lack of dialogue about weight management between PwO and HCPs, and few follow-up appointments may present a challenge to obesity management.
PwO and employers had differing perceptions of the benefit of employer wellness offerings.44
Employers reported the following weight management benefits offered by their companies:

The value of wellness programs offered by employers were perceived differently by employers and PwO.
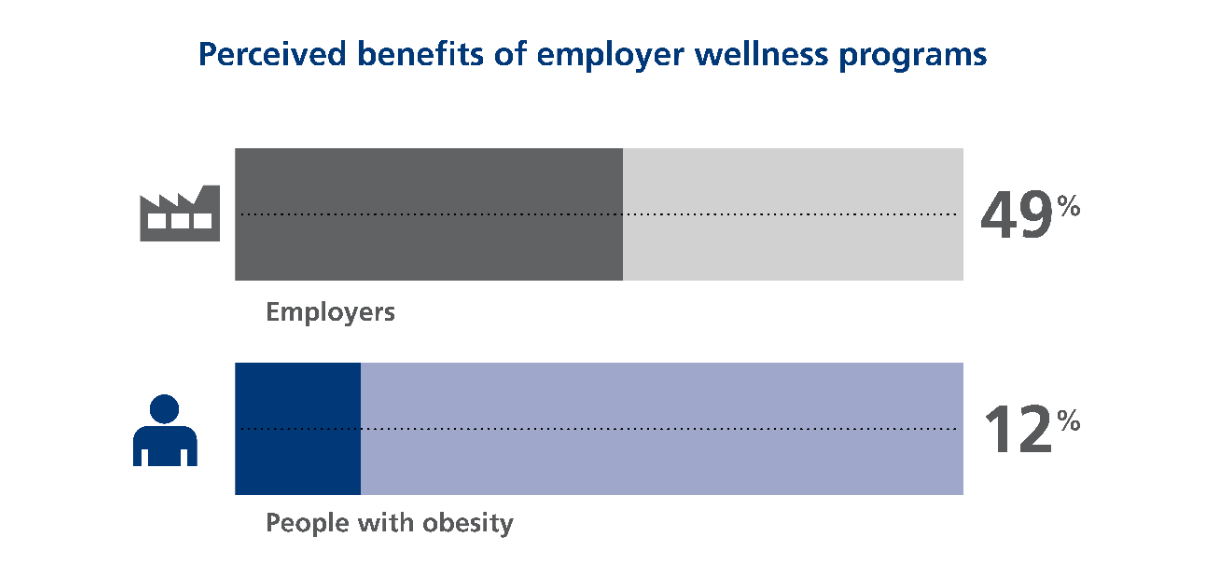
49% of employers believe that wellness programs contribute “significantly” or “a lot” to successful weight loss, whereas only 12% of PwO agreed with these statements.
Perceived reasons for non-participation in employer wellness programs differed between employers and PwO:
Skewed perceptions of the value of wellness programs may present a challenge to effective obesity management.
Obesity should be treated and managed holistically and as a serious chronic disease.11,47
Behavioural and lifestyle interventions:
For obesity, this should include diet, exercise, and behavioural modification.47 Medical nutrition therapy, physical activity, and health behaviour changes are first-line interventions in all individuals with a BMI ≥ 25 kg/m2 and they are recommended as the basis for all obesity management plans.48-50 However, behavioural interventions may not always be sufficient to maintain weight loss and some people living with obesity may require a combination of treatments that includes pharmacotherapy and/or bariatric surgery to help manage their weight.9,43,45
Pharmacotherapy:
For people living with obesity, pharmacotherapy should be considered as a treatment option to decrease weight and improve metabolic and/or health parameters when health behaviour change alone has been ineffective, insufficient, or without sustained benefit.
Based on guideline recommendations, pharmacotherapy can be used for:45
Patients with a BMI of ≥ 30 kg/m2 or ≥ 27 kg/m2 with adiposity-related complications, in combination with medical nutrition therapy, physical activity, and psychological interventions.
Patients with type 2 diabetes and a BMI > 27 kg/m2 for weight loss and glycemic control, in combination with health behaviour changes.
Patients with prediabetes and overweight or obesity (BMI > 27 kg/m2) to delay or prevent type 2 diabetes, in combination with health behaviour changes.
Bariatric surgery:
Bariatric surgery is an intervention for obesity management which is recommended in:51
Patients greater than 18 years of age with a BMI of 35 kg/m², who have at least one major obesity-related complication.
Patients with a BMI between 30–34.9 kg/m² who have been refractory to nonsurgical attempts at weight loss with obesity-related complications, especially type 2 diabetes.
Patients with a BMI ≥ 40 kg/m², independent of the presence of obesity-related complications.
Bariatric surgery requires lifelong medical monitoring and treatment of potential long-term nutritional deficiencies.51,52
For comprehensive medical care of patients with obesity and overweight according to BMI stage.
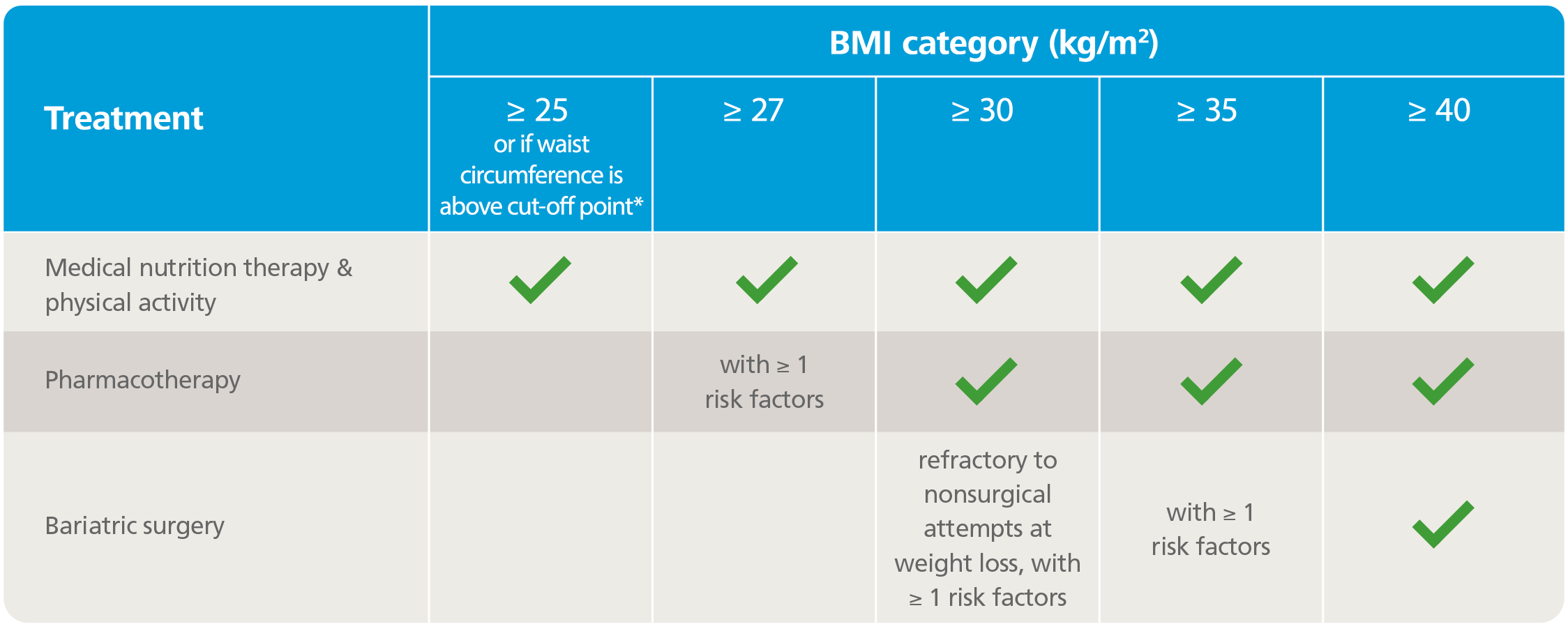
Adapted from Boulé, et al. (2020), Brown, et al. (2020), Glazer, et al. (2020), Pederson, et al. (2020), and Vallis, et al. (2020).
* Body mass index (BMI) and waist circumference cut-off points are different for some ethnic groups; refer to Table 1 of Rueda-Clausen, et al. (2020) for ethnic-specific waist circumference cut-off points.



{kind=link}